A Well-Accepted and Growing Opinion
My approach to strength training is shaped by orthopedic surgery, rehabilitation science, national physical activity guidelines, preventive medicine, and physician-led strength education groups such as Barbell Medicine.
Barbell Medicine has helped explain how strength training fits into real medical care. Their central message is not that everyone needs to become a powerlifter. It is that progressive strength training is one of the most useful, scalable, and underused tools we have for long-term health. Jordan Feigenbaum, MD, MS, and Austin Baraki, MD, are examples of physicians who have brought serious strength training into the medical conversation in a practical, evidence-based way.
I also think often about a lesson I heard from Tedd Mitchell, MD, during my medical training at Texas Tech. The goal of health is not to become the strongest or fastest person in the world, or to chase records forever. The goal is to preserve function, independence, and physical capacity for as much of life as possible. Ideally, we want a long period of high function rather than a long, slow decline.
Strength training is one of the best ways to build that reserve.
The Problem: We Have Underloaded the Population
When people are injured, the natural instinct is often to stop moving, protect the area, and wait until everything feels normal. Terms like rest, immobilization, and activity restriction have long been accepted initial treatments for many injuries.
Sometimes rest and protection are necessary. Certain fractures, tendon repairs, ligament reconstructions, and surgeries have real tissue-healing timelines that need to be respected.
But for many common orthopedic problems, the bigger issue is not that people are doing too much. It is that they have been asked to do too little for too long.
The result is stiffness, weakness, fear of movement, loss of confidence, and a slower return to function.
This can become even more damaging when a highly functional patient gets imaging for one painful area, and the scan shows an “abnormal” finding somewhere else that is not causing symptoms. If the patient is then told to rest, stop activity, or avoid loading the limb because of that incidental finding, we can turn a harmless imaging result into real disability.
The body adapts to what it is repeatedly asked to do. If we ask very little from it, it becomes good at doing very little. If we gradually ask more from it, it usually adapts.
The better default is not reckless activity.
The better default is progressive loading.
The Consequences of Inactivity
Strength is not just a gym topic. It is a health topic.
Most people know they should do some cardiovascular exercise. Far fewer understand that strength training is also part of national health recommendations. Current adult recommendations include 150 minutes of moderate cardiovascular exercise per week, or 75 minutes of vigorous cardiovascular exercise, plus at least two days of muscle-strengthening activity per week. Recent national data suggest only about one-quarter of U.S. adults meet both the aerobic and strength recommendations. Among adults 65 and older, the percentage is even lower.
These recommendations are minimums, not the ceiling. For many people, doing more than the minimum provides additional health benefit, especially when exercise includes meaningful strength training.
The problem is not aesthetics. It is physiology.
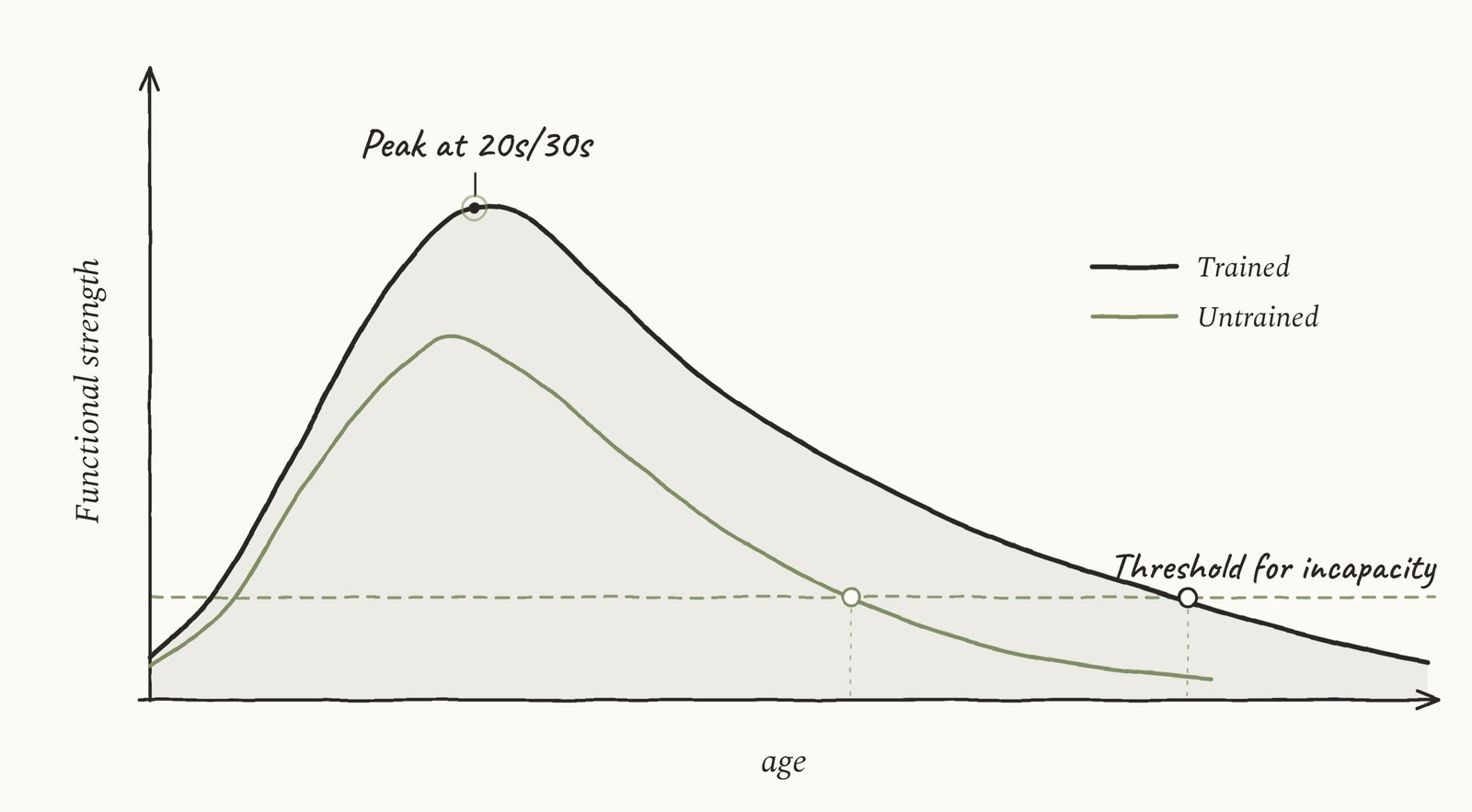
Muscle mass, strength, power, balance, and bone density tend to peak in early adulthood and gradually decline over time. At first, this is easy to ignore. Later, it shows up as difficulty getting out of a chair, trouble climbing stairs, poor balance, falls, fractures, loss of independence, and difficulty recovering from surgery or illness.
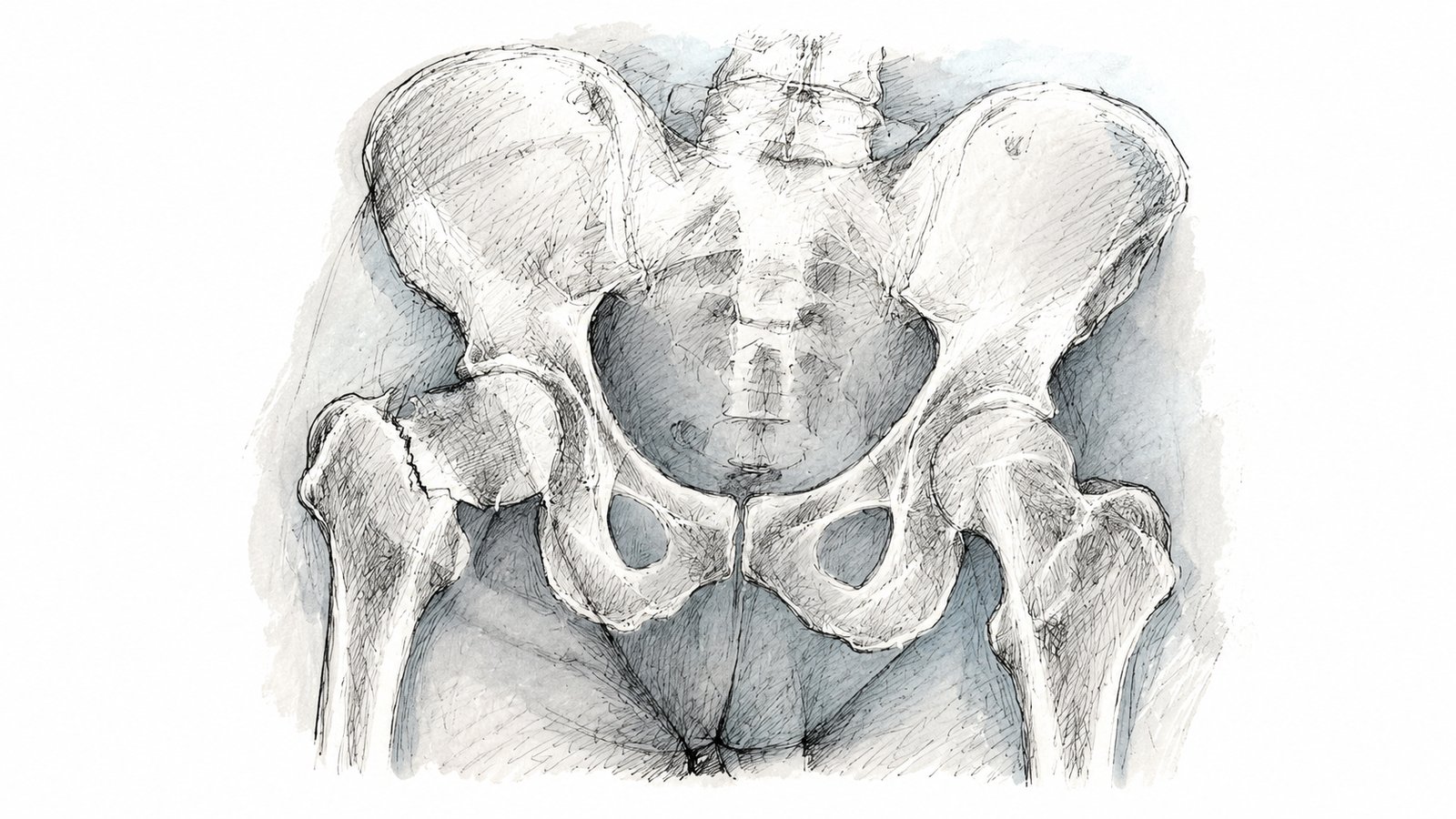
Orthopedic surgeons often see the end stage of this process. A patient falls, breaks a hip, needs surgery, and then struggles to recover because they did not have enough physical reserve before the injury. The fracture is the event, but the loss of reserve was often building for years.
In my experience, this decline often reaches a threshold near the end of life where function suddenly drops off. A person may have been “getting by” for years, but after an illness, fall, fracture, or surgery, there may not be enough reserve left to recover. That can lead to dependence, immobility, and a prolonged final chapter of life that may have been partly preventable.
Strength training is one way to build that reserve and delay, reduce, or sometimes avoid the threshold of immobility and dysfunction.
A Simple, Robust Solution: Lift Heavy Things Progressively
My view is simple: progressive strength training is appropriate for just about everyone.
That includes teenagers, adults, older adults, postmenopausal women, people with arthritis, people recovering from injury, and many who have been told they are “too old” or “too fragile” to lift weights.
The details may change, but the principle does not.
The goal is to expose the body to meaningful force, recover from it, and gradually increase what the body can tolerate.
Most people do not need elaborate restrictions before they start strength training. They need a reasonable starting point, a meaningful load, and a plan to progress.
Heavy is relative. For one person, heavy may mean a barbell deadlift. For another person, heavy may mean standing from a chair while holding a dumbbell. For another, it may mean a slow step-up, a loaded carry, or a controlled squat to a box.
The key is not perfect form, perfect scaling, or the one ideal exercise. The key is lifting something challenging enough to make the body adapt.
Form Matters, But It Is Not Magic
A major barrier to strength training is the fear that imperfect form will automatically cause injury.
That fear is overstated.
Good technique matters. It helps with efficiency, confidence, consistency, and performance. It helps people train harder with less wasted effort. But perfect form is not required before a person is allowed to start getting stronger.
In general media, poor form is often treated as the main reason people get hurt lifting weights. In reality, the bigger problem for most people is that they never lift at all.
Weight training is not uniquely dangerous. Injury rates in weightlifting and powerlifting appear relatively low compared with many common sports and are in the same broad range, or lower, than injury rates reported in some running populations.
That does not mean injury is impossible. It means the fear of lifting is often exaggerated.
For someone new to weight training, there is usually little reason to jump immediately to the heaviest weight they can lift. A smarter approach is to start with a challenging but controlled load, learn the movement, and progress over time.
The body is not fragile. But training works best when the dose is increased gradually.
Loading the Skeleton Matters
One of the clearest examples of the importance of loading the skeleton comes from spaceflight research.
In microgravity, astronauts are removed from the normal loading forces of Earth. NASA notes that weight-bearing bones can lose about 1% of their density per month in space without countermeasures. Because of this, astronauts use resistive exercise devices to load the muscles and skeleton.
This does not mean resistance exercise is the only factor in bone health. Nutrition, hormones, medications, genetics, and other factors matter too. But spaceflight is a dramatic example of a basic principle: the skeleton is designed to respond to load.
Bones, muscles, tendons, and joints need meaningful mechanical stress to maintain and improve capacity.
The principle is the same on Earth: gradually expose the body to a meaningful amount of force, then let it adapt.
Barbells Are Standardized Compound Movements
Barbells are not magic, and they are not required.
But barbell-style training is useful because it is simple, measurable, standardized, and progressive. Squats, deadlifts, presses, rows, and carries train large muscle groups through practical movement patterns.
These exercises can be adjusted by changing the range of motion, load, tempo, number of sets, number of repetitions, weekly frequency, and exercise variation.
The goal is not perfect form forever with light weights.
The goal is competent movement under progressively challenging loads.
While barbell movements are popular and easy to measure, large compound movements can be trained with many tools: dumbbells, kettlebells, machines, sandbags, resistance bands, weighted backpacks, or bodyweight progressions. The tool matters less than the principle.
The muscles and skeleton need to be loaded in a challenging, progressive way.
Why Beginners Can Improve Quickly
Beginners usually do not need a complicated program.
Early strength gains are often neurological. The person is learning the movement, improving coordination, learning how to brace, learning how to produce force, and becoming more comfortable with effort.
That is why people can feel stronger early before they have visibly built much muscle.
The classic strength-training literature supports this idea: early strength gains are often driven heavily by neural factors, with muscle hypertrophy becoming more important after the first several weeks.
This matters for patients because they should not judge a strength program after one or two weeks. The first several weeks are often about learning, coordination, confidence, and consistency. More visible muscle and tissue adaptation takes longer.
You do not need to feel transformed immediately. You need to stay with the program long enough for your body to adapt.
Perceived Exertion: How Hard Should It Feel?
You do not have to max out to get stronger.
A practical target is to finish most working sets feeling like you could have done about 2 to 4 more good repetitions if you absolutely had to.
That means the set was challenging, but controlled.
This is often discussed in strength training as “rate of perceived exertion,” or RPE. A simple way to understand RPE is to ask how many good repetitions you had left at the end of a set. This is sometimes called “reps in reserve.”
For example:
- If you finish a set and could have done 4 more good reps, that is about a 6 out of 10 effort.
- If you could have done 3 more good reps, that is about a 7 out of 10 effort.
- If you could have done 2 more good reps, that is about an 8 out of 10 effort.
- If you could have done 1 more good rep, that is about a 9 out of 10 effort.
- If you could not have done another rep, that is a 10 out of 10 effort.
Most beginners do not need to train at a 10 out of 10 effort. The majority of growth at any experience lives around a 6 to 8 out of 10 effort. That is hard enough to create adaptation, but not so hard that every workout becomes a test of survival.
For many patients, a good starting prescription is three sets of a squat pattern, a hinge or deadlift pattern, and an upper-body push or pull pattern, performed a few times per week.
The exact exercise matters less than the principle: train the major movements, use enough effort to create adaptation, and progress gradually.
What I Want Patients to Understand
Strength training is not only for athletes.
Strength is functional reserve. Reserve is what lets you handle injuries, surgery, aging, falls, and the physical demands of life.
You do not need to become a powerlifter. You do need to challenge your muscles.
The safest long-term plan is usually not avoiding load forever. It is learning how to load your body consistently, intelligently, and progressively.
Start where you are. Train the major movements. Lift something challenging. Repeat it long enough for your body to adapt.
References
- Barbell Medicine. The Team. Barbell Medicine. Accessed June 27, 2026.
- Texas Tech University System. Tedd L. Mitchell, M.D. Texas Tech University System. Accessed June 27, 2026.
- Centers for Disease Control and Prevention. Adding Physical Activity as an Adult. CDC. Updated December 4, 2025. Accessed June 27, 2026.
- Office of Disease Prevention and Health Promotion. Increase the proportion of adults who do enough aerobic and muscle-strengthening activity — PA-05. Healthy People 2030. Accessed June 27, 2026.
- National Aeronautics and Space Administration. Counteracting Bone and Muscle Loss in Microgravity. NASA. Published December 1, 2023. Accessed June 27, 2026.
- Sibonga J, Matsumoto T, Jones J, et al. Resistive exercise in astronauts on prolonged spaceflights provides partial protection against spaceflight-induced bone loss. Bone. 2019;128:112037. doi:10.1016/j.bone.2019.07.013.
- Moritani T, deVries HA. Neural factors versus hypertrophy in the time course of muscle strength gain. American Journal of Physical Medicine. 1979;58(3):115-130. PMID:453338.
- Helms ER, Cronin J, Storey A, Zourdos MC. Application of the repetitions in reserve-based rating of perceived exertion scale for resistance training. Strength and Conditioning Journal. 2016;38(4):42-49. doi:10.1519/SSC.0000000000000218.
- Tung MJY, Chua JYX, Goh GSL, et al. Injuries in weightlifting and powerlifting: an updated systematic review. BMJ Open Sport & Exercise Medicine. 2024;10(4):e001884. doi:10.1136/bmjsem-2024-001884.
- Videbæk S, Bueno AM, Nielsen RO, Rasmussen S. Incidence of running-related injuries per 1000 h of running in different types of runners: a systematic review and meta-analysis. Sports Medicine. 2015;45(7):1017-1026. doi:10.1007/s40279-015-0333-8.
- Faigenbaum AD, Kraemer WJ, Blimkie CJR, et al. Youth resistance training: updated position statement paper from the National Strength and Conditioning Association. Journal of Strength and Conditioning Research. 2009;23(5 Suppl):S60-S79. doi:10.1519/JSC.0b013e31819df407.